The prestigious New England Journal of Medicine has sullied its reputation, publishing a study claiming to show a link between an intact penis and cervical cancer in the partner, carried out over five countries. The study is flawed in a variety of ways, detailed below.
|
"Today many investigators use a statistical software package without really understanding what it does. You can just enter data, and press a button to select a program. As a result, some research seems quite mindless. It looks for associations, without having any theoretical model in mind at all.... The situation is sometimes even worse with more sophisticated statistical techniques contained in easy-to-use software packages. Often people who use them have no idea what the packages are for." - Ian Hacking, Probability and Inductive Logic, 2001, pp217-218 "...the statistical methods currently used throughout the scientific community ... grossly exaggerate both the size of implausible effects and their statistical significance, and lend misleading support to entirely spurious 'discoveries'. [...] The result has been an ever-growing number of spurious claims... and continuing disappointment as supposed breakthroughs fail to live up to expectations." - Robert Matthews The use and abuse of subjectivity in scientific research |
|
The New England Journal of Medicine Volume 346:1105-1112 April 11, 2002 Number 15 Male Circumcision, Penile Human Papillomavirus Infection, and Cervical Cancer in Female Partners Xavier Castellsagué, M.D., F. Xavier Bosch, M.D., Nubia Muñoz, M.D., Chris J.L.M. Meijer, Ph.D., Keerti V. Shah, Dr.P.H., Silvia de Sanjosé, M.D., José Eluf-Neto, M.D., Corazon A. Ngelangel, M.D., Saibua Chichareon, M.D., Jennifer S. Smith, Ph.D., Rolando Herrero, M.D., Victor Moreno, M.D., Silvia Franceschi, M.D., for the International Agency for Research on Cancer Multicenter Cervical Cancer Study Group ABSTRACT Background Methods Results Conclusions Since Hutchinson reported in 1855 that circumcision might prevent syphilis,1 studies have suggested that circumcision may reduce the risk of penile cancer, urinary tract infections, and common sexually transmitted diseases, including human immunodeficiency virus (HIV) infection.2,3,4,5,6,7,8,9 [No mention of the many studies that contradict these, nor the many since Hutchinson that promoted circumcision as a preventative of masturbation, TB, epilepsy, etc.] Little is known, however, about the effect [if any] of male circumcision on the risk of acquiring human papillomavirus (HPV). HPV causes genital warts in men and women, and it has been linked to cancers of the cervix, vulva, vagina, anus, and penis.10,11 Cervical cancer is the second most common cancer among women worldwide, and up to 99 percent of all cases may be attributed to infection by oncogenic HPV genotypes.12,13 [This statement is reminiscent of retailers offering price reductions of "up to 50%".] Therefore, factors that reduce the probability of acquiring or transmitting HPV among men or women may reduce the risk of disease associated with these infections.
During the past 15 years the International Agency for Research on Cancer has performed several large casecontrol studies of cervical cancer in different countries. We used data from these studies to assess the effect of male circumcision on the risk of genital HPV infection in the men themselves and the risk of cervical cancer in their sexual partners. Methods Study Design Study subjects were enrolled in one of seven casecontrol studies, five involving invasive cervical cancer and two involving cervical carcinoma in situ. The fieldwork for these studies was conducted from 1985 through 1993. Two studies each were conducted in Spain and Colombia, and one study each was conducted in Brazil, Thailand, and the Philippines. [Of those, circumcision is common only in the Philippines. Any of a huge variety of differences between countries could be responsible for any difference.] Details of the methods of each study, as well as the results of analyses of some risk factors for cervical cancer, have been published previously.14,15,16,17,18,19,20,21,22,23 Female patients were women who had newly diagnosed, histologically confirmed cervical carcinoma in situ or invasive cervical cancer. Control women were recruited from the general population in the two studies of invasive cervical cancer in Spain and Colombia (population-based studies) and from the same hospitals as the patients in the case of the other studies (hospital-based studies). In all studies, control women were frequency-matched to the women with cervical cancer according to age. [they could not have been matched with women in their own countries, since the number of controls varied widely] Since male and female risk factors for carcinoma in situ were similar to those for invasive cervical cancer, women with carcinoma in situ and controls were also included in the present analysis.24 Men who were eligible for the present study were the husbands or stable partners of the women with cervical cancer and the control women enrolled in each of these studies. A man was considered to be a stable partner of an enrolled woman if he reported having had regular sexual intercourse with the woman for at least six months, whether or not they were married or lived together. [This gives him very little time to infect her with HPV and for it to have given her cervical cancer.] All protocols were approved by the International Agency for Research on Cancer and the local ethics and research committees. Informed consent was obtained from all study subjects. Oral consent was obtained from the subjects in the Spanish and Colombian studies (which were initiated in 1985), consistent with the standard at the time. In the remaining studies, which were initiated later, written informed consent was obtained. Questionnaire and Medical Examination Subjects were interviewed with use of a standardized questionnaire administered in person by specially trained interviewers. Detailed information was collected on demographic and socioeconomic variables, sexual history, and circumcision status. Detection of HPV DNA Two samples of exfoliated cells were obtained from the penis: one from the distal urethra with the use of a very thin, wet, cotton-tipped swab and one from the external surface of the glans and coronal sulcus with the use of a standard-sized wet, cotton-tipped swab. [The authors present no evidence that the distal urethra or the glans/coronal sulcus are the only or most likely sites of HPV carriage or transmission, and HPV can be visible or detectable anywhere on the genitals. It could be just as easily transmitted from the scrotum or pubic area. The second site is very different in intact and circumcised men, so it should come as no surprise that virus was detected more often from the moist surface of the intact men's penises using this method - but it doesn't follow that more intact men carried the virus. To determine whether circumcision had an effect on HPV status, a circumcision-neutral site was necessary.] Cervical exfoliated cells were collected from the women as previously described.14,15,16,17,18,19,20 The detailed protocol used for the polymerase-chain-reaction (PCR) assay for the detection of HPV DNA in the cervical and penile specimens has been described previously.14,15,16,17,18,19,20,21,22,23 Briefly, the L1 consensus primers MY09MY11, as modified by Hildesheim et al.,25 were used for the samples collected in the Colombian and Spanish studies. The GP5+/6+ general primer system was used for the samples collected in the remaining studies. PCR products were assessed for HPV DNA with the use of a cocktail of HPV-specific probes and were genotyped by hybridization of the PCR products with type-specific probes for 33 HPV types in the case of cervical samples and for at least 6 HPV types (6, 11, 16, 18, 31 and 33) in the case of penile samples.26,27 Samples that were positive for HPV but that did not hybridize with any of the type-specific probes were called "HPV X." Amplification of a fragment of the -globin gene served as an internal quality control for each specimen. Statistical Analysis We used unconditional logistic regression to estimate odds ratios and 95 percent confidence intervals in order to measure associations between specific variables and the risk of penile HPV infection or cervical cancer. All logistic-regression models were adjusted for the age of the male partner (in quartiles) and the study in which his partner was enrolled (seven categories). Covariables in the model for penile HPV infection included the male partner's level of education (primary school or less vs. secondary school or higher), the age at which he first had sexual intercourse (16, 17 to 18, or 19 years), his lifetime number of sexual partners (1 to 5, 6 to 20, or 21), and his self-reported frequency of genital washing after intercourse (always vs. occasionally or never [What would a man who washed "often" or "sometimes {about half the time}" answer?]). The Wald test, adjusted for the same covariables, was used to assess the association of each variable with circumcision status. Further adjustment for casecontrol status or the presence of cervical HPV DNA did not substantially alter the point estimates, and these variables were not included in the analyses. Logistic-regression models for cervical cancer were also adjusted for the woman's age, her lifetime number of sexual partners, and the age at which she first had sexual intercourse. Fisher's exact test was used to assess the association between male circumcision status and the risk of penile HPV infection, with stratification according to several characteristics of the men. [Hacking's and Matthews' warning against the misuse of statistics is very relevant here.] We assessed whether the association of circumcision status with the risk of penile HPV infection and cervical cancer differed significantly according to the country in which the various studies were conducted by including in the fully adjusted logistic-regression model an interaction term combining country and circumcision status. A two-sided P value of less than 0.05 was considered to indicate statistical significance.
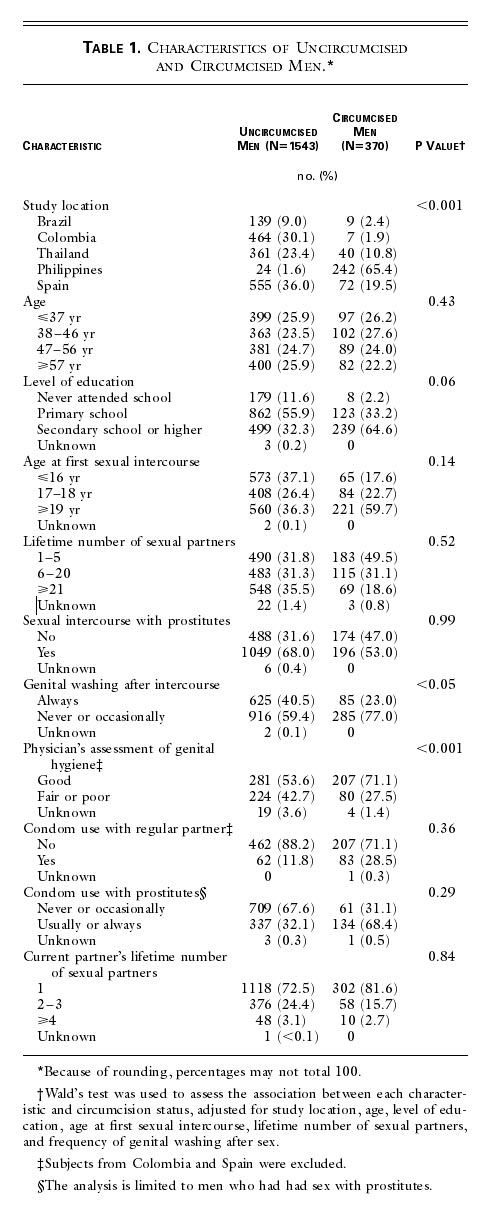
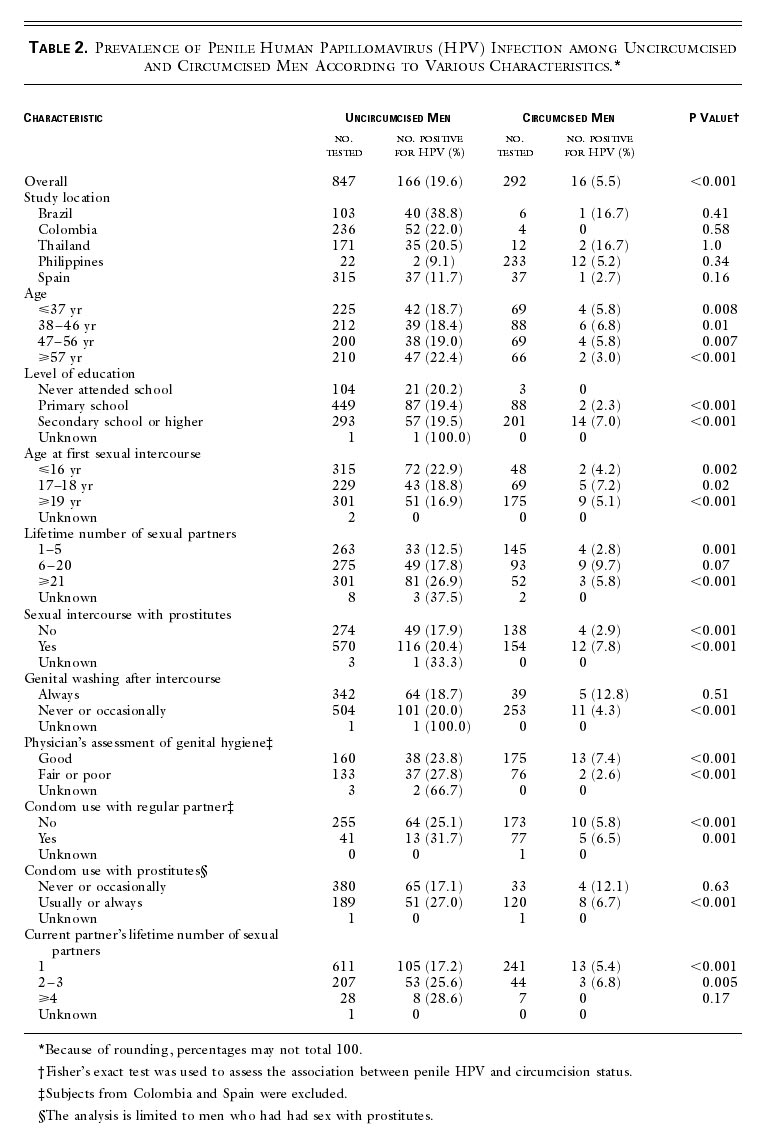
Results Study Subjects Of the 3790 women (1896 women with cervical cancer and 1894 controls) who were enrolled in the seven casecontrol studies, 2800 (1329 women with cervical cancer and 1471 controls) reported having a husband or stable male partner at study entry. A total of 984 of the 1329 partners of women with cervical cancer (74.0 percent) and 937 of the 1471 partners of control women (63.7 percent) were interviewed. Of these, 807 partners of patients (82.0 percent of those interviewed) and 717 partners of control women (76.5 percent) provided cytologic specimens, of which 610 (75.6 percent) and 533 (74.3 percent), respectively, yielded a valid PCR result. Eight men whose circumcision status was unknown (four with a valid PCR result and four who did not provide samples) were excluded from the analyses. [This whittling down of the numbers - from 3790 women down to 1143 partners - does not occur in a random way. These non-response figures influence the results in an unmeasured way, making statisticians suspicious of this kind of study.] Overall, the men whose HPV status could be confirmed by PCR assay were similar to the men whose HPV status could not be established with respect to age, level of education, circumcision status, and variables related to sexual behavior. In Colombia, highly educated men were more likely than less educated men to have a valid PCR result. In Thailand, uncircumcised men and men who reported having had a large number of sexual partners were more likely to have a valid PCR result than their counterparts. [There were only 40 circumcised "counterparts" in the Thai sample.] However, the exclusion of men from Thailand did not substantially alter the magnitude of the associations. Women whose partners participated in the study did not differ significantly from women whose partners did not participate with respect to age, level of education, or variables related to sexual behavior. Likewise, women whose partners were tested for HPV infection were similar to those whose partners were not tested. Characteristics of the Subjects The overall prevalence of self-reported circumcision was 19.3 percent (370 of 1913 men): 1.5 percent in Colombia [ie, hardly any], 6.1 percent in Brazil, 10.0 percent in Thailand, 11.5 percent in Spain [very few], and 91.0 percent [the great majority] in the Philippines. [So what purports to be a comparison of circumcision status is actually a comparison of countries.] As compared with uncircumcised men, circumcised men had a higher level of education, were less likely to report frequent genital washing after sex, [i.e. men in the Philippines differed in these ways from men in the other countries.] and were more likely to have good genital hygiene, as assessed by a physician (Table 1). [How much of that was physicians' perceptions of intact genitals as intrinsically less clean than circumcised?] View this table: [in this window] [in a new window] Table 1. Characteristics of Uncircumcised and Circumcised Men. [The table shows a perfectly baffling array of characteristics that have significant differences between cut and intact men - most probably because of the different countries they live in. They include sex with prostitutes, education, age at first intercourse, and use of condoms. The authors are simply fooling themselves if they think they can pool all this data and then correct for these differences, and others they have not considered, by statistical manipulation.] Circumcision and Penile HPV Infection HPV DNA was detected in 182 of the 1139 penile specimens (16.0 percent). The most common HPV genotypes were 16 (24.7 percent of all positive samples), 18 (4.9 percent), 6 or 11 (3.3 percent), 53 (3.3 percent), 31 (2.7 percent), and 33 (2.2 percent). The type could not be identified in the case of 51.1 percent of the positive samples. HPV types 35, 39, 45, 51, 52, 54, and 59 each accounted for less than 1.5 percent of the positive samples. HPV was detected in 19.6 percent of uncircumcised men (166 of 847) and 5.5 percent of circumcised men (16 of 292). As compared with uncircumcised men, circumcised men had a lower prevalence of HPV infection [detected] in all subgroups defined according to base-line characteristics [This might seem to mean that the "effect" of circumcision was more important than those characteristics, but it really just means that the effect of living in the Philippines was more important.] (Table 2). View this table: [in this window] [in a new window] Table 2. Prevalence of Penile Human Papillomavirus (HPV) Infection among Uncircumcised and Circumcised Men According to Various Characteristics.
The overall odds ratio for penile HPV infection associated with self-reported circumcision was 0.37 (95 percent confidence interval, 0.16 to 0.85), after adjustment for age, study location, level of education, age at first sexual intercourse, lifetime number of sexual partners, and frequency of genital washing after sex. The adjusted odds ratio associated with clinician-assessed circumcision was 0.44 (95 percent confidence interval, 0.17 to 1.13 [When the 95% confidence interval is greater than 1.0, there may be no statistical significance.]). There was an inverse association between circumcision and the risk of HPV infection in all studies (P for heterogeneity=0.87), and this finding persisted whether or not the female partner had cervical HPV infection or had been given a diagnosis of cervical cancer (data not shown). The only other risk factor that was significantly associated with the risk of penile HPV infection was the number of sexual partners the men had had; as compared with men who had five or fewer partners, those who had had six or more partners had an odds ratio of 2.0 (95 percent confidence interval, 1.3 to 3.2). The odds ratio for HPV infection among circumcised men, as compared with uncircumcised men, was similar after the exclusion of men from Spain and Colombia; these men did not undergo a medical examination of the penis (odds ratio, 0.56; 95 percent confidence interval, 0.20 to 1.56 [i.e. no significance]). The odds ratio was also not changed significantly by the exclusion of men from the Philippines, who represented 65.4 percent of all circumcised men in the study (odds ratio, 0.32; 95 percent confidence interval, 0.11 to 0.93).
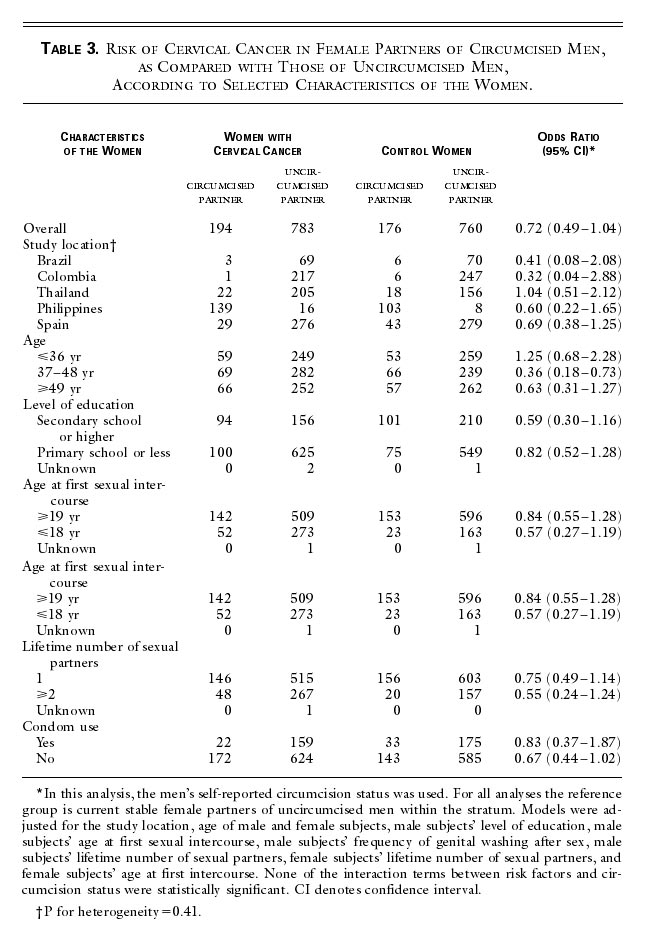
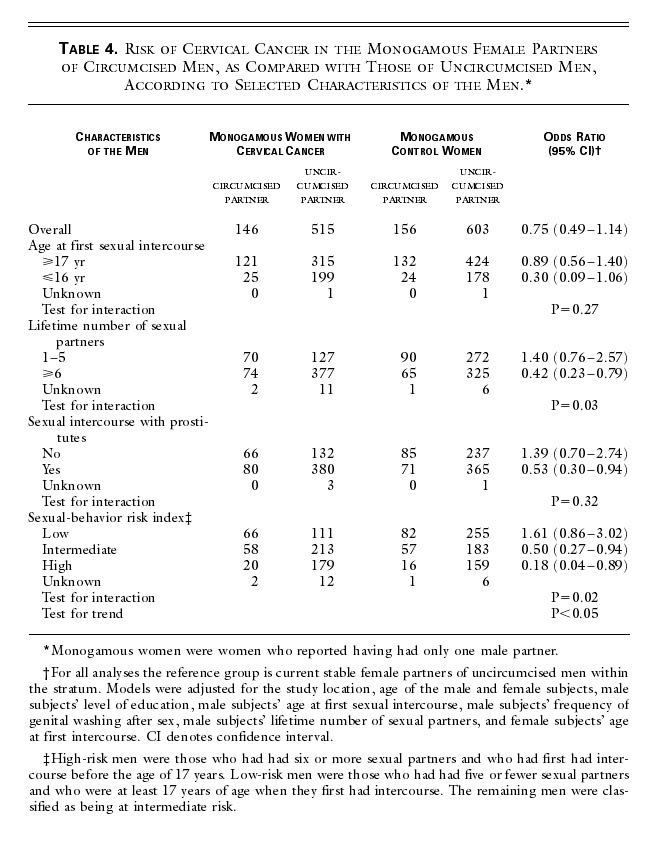
Circumcision and Cervical Cancer Male circumcision was associated with a moderate, but nonsignificant, decrease in the risk of cervical cancer in the men's female partners (odds ratio for self-reported circumcision, 0.72; 95 percent confidence interval, 0.49 to 1.04 [i.e. no significance]; odds ratio for clinician-confirmed circumcision, 0.69; 95 percent confidence interval, 0.43 to 1.11 [i.e. even less likelihood of significance]). There was no evidence of heterogeneity with respect to the location of the study (P=0.41), [This seems to refer to some kind of statistical manipulation of the data after they had pooled data from the different countries, none of which individually showed any correlation between circumcision and cervical cancer.] and the inverse association was not substantially altered by any of the characteristics of the women that we assessed (Table 3). Results were similar after the exclusion of men from Spain and Colombia (odds ratio, 0.79; 95 percent confidence interval, 0.47 to 1.33) and after the exclusion of men from the Philippines (odds ratio, 0.76; 95 percent confidence interval, 0.51 to 1.15). [Again, there is no need to exclude countries when the unpooled data from the separate countries is available.] View this table: [in this window] [in a new window] Table 3. Risk of Cervical Cancer in Female Partners of Circumcised Men, as Compared with Those of Uncircumcised Men, According to Selected Characteristics of the Women. [This table shows that the control group in the Philippines was only 111 couples, much smaller than the cervical cancer group (155 couples). The Philippines was the prime source of circumcised men. The essence of case-control studies is that the control group matches the case group as far as possible except in the variable being tested. It is not acceptable to use "controls" taken from another study in another country. Doing so greatly reduces the significance of the results.] To minimize confounding as a result of the women's having had male partners other than the current partner, we restricted the analysis to the 1420 men whose female partner reported having had only one sexual partner. [Cultural differences mean women in different countries may have been more or less ready to report having had other partners.] We also stratified this analysis according to several variables related to the male partner's sexual behavior in order to test the hypothesis that the reduction in the risk of cervical cancer would be greater among women whose male partners were at higher risk for HPV infection. As one measure of risk, we computed an index based on a man's age when he first had sexual intercourse and his total number of sexual partners. [ Early first intercourse does of course increase the time available to have more partners, but why should it increase the risk of HPV independent of the number of partners? The authors are data-mining.] Men who had had six or more sexual partners and who had first had intercourse before the age of 17 years were considered to be at high risk; men who had had five or fewer sexual partners and who were at least 17 years of age when they first had intercourse were considered to be at low risk; and the remaining men were classified as being at intermediate risk. [Did the authors devise this "high risk" characteristic before or after finding it associated with circumcision status?] The inverse relation between circumcision and the risk of cervical cancer [did not exist for women whose partners had had few other partners, but] was stronger and was significant in the case of women whose partners had a high risk index and [they mean, "that is"] who engaged in sexual practices known to increase the risk of exposure to HPV, such as having had intercourse before the age of 17 years, having had six or more sexual partners, and having a history of contact with prostitutes (Table 4). Tests for an interaction between circumcision status and the male partner's number of sexual partners and between circumcision status and the risk index were significant (P=0.03 and P=0.02, respectively). [Circumcised men who used prostitutes were more likely to use condoms than intact men. This would affect HPV rate.] View this table: [in this window] [in a new window] Table 4. Risk of Cervical Cancer in the Monogamous Female Partners of Circumcised Men, as Compared with Those of Uncircumcised Men, According to Selected Characteristics of the Men. Discussion In our study, male circumcision was associated with a reduced risk of penile HPV infection in men. [..."associated" through the accident of living in the Philippines.] We also found an inverse association between circumcision and the risk of cervical cancer was significant among women whose male partners engaged in sexual practices known to increase the risk of infection with HPV, such as having had multiple sexual partners. [What they did NOT find was an association between intact partners and cervical cancer.] The assessment of the reliability and validity of self-reported circumcision status has yielded inconsistent results,8,28,29,30 and potential misclassification of circumcision status with the use of this method has been a major concern in previous studies. One strength of our study is the high rate of accuracy of self-reported circumcision status. Medical examination of the penis, performed in 43 percent of the men, confirmed the self-reported circumcision status in 95 percent of those examined. [Since fewer than half were examined, the accuracy of self-reporting may be somewhat less than 95%, and then the statistical effects of mis-assignment destroy the slim margins of confidence in the other measures shown here.] Inverse associations with the risks of penile HPV infection and cervical cancer were similar when circumcision status was classified according to self-report or medical examination. Likewise, the exclusion of subjects who had not undergone a penile examination (men from Spain and Colombia) did not materially affect the findings. [Wynder and Licklider reported that 24% of 200 male patients were unable to correctly state their own circumcision status (Wynder EL, Licklider SD. The question of circumcision. Cancer. 1960; 13:442-5).]
A potential concern with respect to our study was the fact that 65 percent of the circumcised men were from the Philippines. This result was not unexpected, since mass circumcision sessions are regularly conducted by many organizations in that country and most boys are circumcised before puberty. We performed a secondary analysis excluding men from this study site and found that results were virtually unchanged. [So they pooled the data that showed no significant correlations in the countries taken separately, and then "performed a secondary analysis" on the pooled data. This suggests they were determined to find a correlation at all costs.]
Some studies have reported that genital warts are more common among uncircumcised men than among circumcised men,4,5,30,31,32,33 but other studies have not confirmed these associations.2,34,35,36,37 Epidemiologic evidence suggests that the absence of circumcision at birth and the presence of phimosis, poor genital hygiene, genital warts, and HPV infection are risk factors for penile cancer.3,10,11,38,39 Other data have suggested that the risk of cervical cancer is reduced among the female partners of circumcised men, but these studies were limited by the small number of circumcised men or the low sensitivity of the methods used to detect HPV DNA.40,41,42 Little is known about the mechanisms by which removal of the foreskin may protect against HPV infection. [The authors are confusing correlation with causation.] Our data suggest that, even though circumcision increases the probability of maintaining good penile hygiene, there are other ways in which circumcision reduces the risk of penile HPV infection. The penile shaft and the outer surface of the foreskin are covered by a keratinized stratified squamous epithelium that provides a protective barrier against HPV infection. In contrast, the mucosal lining of the prepuce is not keratinized and may be more vulnerable to the virus.43 Since during intercourse the foreskin is pulled back, the inner mucosal surface of the prepuce is wholly exposed to vaginal secretions. HPV might be afforded access to the basal cells through minute ulcers or small epithelial abrasions.44 Removal of the foreskin could minimize the probability of viral entry by markedly decreasing both the size of the surface area vulnerable to HPV and the likelihood of mucosal trauma during intercourse. The glans of a circumcised penis has a thicker, cornified epithelium, making it more resistant to abrasions and less susceptible to the entry of HPV [or to nervous stimulation]. The only mucosal epithelium in a circumcised penis is in the distal urethra, a site known to contain comparatively few HPV-related lesions.33 Our finding that male circumcision may reduce the risk of cervical cancer in female sex partners is highly plausible for several reasons. First, circumcision is associated with a significant decrease in the risk of penile HPV infection. Second, and as indicated in further analyses of the same data, penile HPV infection is associated with a fourfold increase in the risk of cervical HPV infection in the female partner (data not shown). Third, cervical HPV infection is associated with a 77-fold increase in the risk of cervical cancer (data not shown). In conclusion, our study has provided epidemiologic evidence that male circumcision is associated with a reduced risk of genital HPV infection in men and with a reduced risk of cervical cancer in women with high-risk sexual partners. Thus, circumcision can be considered an important cofactor in the natural history of HPV infection, since it may influence the risks of the acquisition and transmission of HPV as well as of cervical cancer. These findings are consistent with those of other studies that male circumcision is associated with a reduced risk of HIV infection,7,8,9 penile cancer,2,3 and a number of other common sexually transmitted diseases.4,5 Given the worldwide effect of these diseases on public health, further study is needed to determine whether routine circumcision can reduce the risks of HIV and HPV infections and other sexually transmitted diseases. ["And therefore Carthage must be destroyed." - Cato
And if female genital modification were found to reduce the incidence of HPV or cervical cancer...?
"If you are an intact male, have had lots of unprotected sex with lots of different women and marry a virgin, your wife may have a real but statistically insignificant increased chance of getting HPV." - Dr Dean Edell
Some time ago, Indian research showed that the subpreputial moisture
contains lysozyme, an enzyme that has anti-bacterial and anti-viral
properties. That file is available on line.
Later Fleiss, Hodges, and Van Howe studied the immunological functions of
the prepuce. That paper is also online.
Genital warts are also caused by HPV, although a different strain from the
strain that cause cervical cancer, and circumcised men are more likely to have genital warts than uncircumcised men.
] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
The New England Journal of Medicine April 11, 2002 Male Circumcision, Penile Human Papillomavirus Infection, and Cervical Cancer It is uncertain whether male circumcision reduces the risk of penile human papillomavirus (HPV) infection and of cervical cancer in a man's female partner. The authors studied women and their male partners enrolled in seven casecontrol studies of cervical carcinoma in situ and cervical cancer in five countries in Europe, South America, and Asia. Circumcised men were significantly less likely than uncircumcised men to have penile HPV infection. Women whose partners had six or more lifetime sexual partners were less likely to have cervical cancer if their partners were circumcised than if they were uncircumcised. These data suggest that male circumcision may reduce the risk of penile HPV infection in men and the risk of cervical cancer in female partners of sexually promiscuous men. Related Editorial The New England Journal of Medicine Editorial Volume 346:1160-1161 April 11, 2002 Number 15 Cervical Cancer and the Elusive [or Illusory] Male Factor Male circumcision is probably one of the oldest surgical procedures [As a general rule, articles that begin by citing the great antiquity of circumcision are biased in its favour. Calling ritual circumcision a "surgical procedure" is like calling cutting a hole in the skull to release evil spirits "cranial surgery".] and is still the most common. Globally, about one man in four is likely to undergo circumcision for various reasons.1 In the United States, an estimated 80 percent of all newborn boys were circumcised in the 1970s. These rates have subsequently decreased, however, as a result of several policy statements issued by the American Academy of Pediatrics. According to the most recent of these documents, the medical benefits are "not sufficient to recommend routine neonatal circumcision."2 Notwithstanding this balanced statement, it is generally accepted that circumcision may reduce the prevalence and thereby the sexual transmission of several infectious diseases. [But even if this were granted, from what level to what level, and is that difference worth it?] Of the various infectious agents involved,1 certain oncogenic subtypes of human papillomavirus (HPV) are directly linked to some genital cancers and are considered to be the main cause of both premalignant and malignant lesions of the uterine cervix. The article by Castellsagué and colleagues3 in this issue of the Journal represents the culmination of a major research effort undertaken by the International Agency for Research on Cancer to evaluate the role of HPV and various modifying factors in the development of cervical cancer. In the context of this large project, seven casecontrol studies were undertaken in five countries on three continents [...none of them countries where the numbers of circumcised and intact men are comparable...]. Using results from all seven studies, Castellsagué et al. report two main findings that are ostensibly interrelated: male circumcision is associated with a reduced risk both of penile HPV infection and of cervical cancer in the female partners of men who had six or more lifetime sexual partners.
That circumcision may reduce the risk of cervical cancer in the female partner has long been suspected.4 However, until certain types of HPV were conclusively implicated in the etiologic process of this cancer, the reason underlying the reduced risk remained poorly understood. The convincing evidence provided by Castellsagué and colleagues that the prevalence of HPV infection is reduced among circumcised men clarifies the nature of the elusive male factor5 in the causation of cancer of the cervix and provides a biologically plausible [but not convincing] explanation for the overall excess risk of cervical cancer among female partners of uncircumcised men. The study has several strengths: it was large, used state-of-the-art laboratory procedures for the detection of HPV infection [but an unbalanced method of collecting samples], and included several different populations, a factor that enhances the generalizability of the results. [But it introduces new, trans-national, confounding factors.] The integration of molecular techniques and epidemiologic methods produced a powerful composite tool for the study of the etiologic process of cervical cancer. However, the shortcomings of the study should also be recognized. Because many factors associated with HPV infection are also more common among uncircumcised than circumcised men, such as a history of multiple sexual partners and poor genital hygiene, these factors may help to explain the results of the study. That confounding was important is demonstrated by the finding that strong associations in the crude data between circumcision and penile HPV infection and between circumcision and cervical cancer in a man's female partner were attenuated after adjustment for these and other factors [...suggesting that adjustment for all relevant factors would "attenuate" them altogether]. Appropriate statistical techniques were used to adjust for confounding. Nonetheless, when variables are difficult to define and measure accurately (such as the frequency of genital washing after intercourse or the general adequacy of a subject's genital hygiene judged on the basis of a single assessment), they are also difficult to control for. Another, probably unavoidable, limitation was the way in which the factor of main interest ‹ circumcision ‹ was ascertained. [They were able to ascertain it definitively in nearly half the cases and found a significant error in self-reporting, significantly loaded in one direction, which they chose to disregard. It could have been avoided by examining all the men in the study.] Progression from infection with an oncogenic HPV to the development of carcinoma in situ and, ultimately, to invasive cervical cancer may take several decades.6 Because of this long latency, the possibility that the female partner may have become infected with HPV many years earlier by a different male partner cannot be ruled out. Castellsagué et al. appropriately limited their analyses to the husbands or stable partners of the women, but misclassification would tend to attenuate [or exaggerate] the true association between circumcision and the risk of cervical cancer, and the reduction in risk among the female partners of circumcised as compared with uncircumcised men may well be more substantial than reported [or less substantial, or completely insubstantial]. With respect to the public health implications of this study, it is important to emphasize that circumcision itself does not protect against cervical cancer. Rather, circumcision should be considered as a modifying factor, in that it protects against cervical cancer by reducing the prevalence of the principal cause, HPV infection. In other words, in the absence of penile infection with an oncogenic HPV strain, circumcision should have no effect on the female partner's risk of cervical cancer. In this regard, the lower incidence of cervical cancer was limited to the female partners of circumcised, as compared with uncircumcised, men who also had six or more lifetime sexual partners. As Castellsagué et al. indicate, circumcision of men at high risk for penile HPV infection may reduce the overall risk of cervical cancer among their female partners by 50 percent or more. If we assume that 25 percent of men around the world are circumcised,1 then the general adoption of circumcision might lead to a further reduction in the incidence of cancer of the cervix of 23 to 43 percent. [This is a wild assumption, not good statitistics - but it has been widely publicised.] Because circumcision also tends to reduce the risk of penile cancer,7 human immunodeficiency virus infection,8 and perhaps other urogenital infections,8 this practice should have considerable public health benefits. These implications need, however, to be considered in the broader context of costs and feasibility [and ethics and human rights - and grave doubts about the claimed correlation]. Although carcinoma of the cervix remains one of the leading causes of death from cancer among relatively young women, notably in developing countries,9 numerous approaches could change this gloomy picture. In Sweden, for example, earlier clinical detection of invasive cancer, achieved through increased public and professional awareness, combined with ready access to basic treatment, reduced the five-year case fatality rates from about 80 percent to 40 percent between 1920 and 1960. Indeed, before this intervention, the situation in Sweden was similar to that in many poor countries, where most cervical cancers are diagnosed in advanced, incurable stages.6 With more resources and a sophisticated infrastructure, the incidence of cervical cancer and the associated mortality can be further reduced by detecting and eliminating precursor lesions, chiefly carcinoma in situ. Since the mid-20th century, cytologic screening with use of the Papanicolaou test has achieved this aim in many developed countries,6 and HPV testing may soon become a complementary tool. [The new vaccine against cervical cancer ckould be another factor.] Regular use of condoms may also inhibit sexual transmission of HPV and thereby prevent cervical cancer. The use of condoms can, at least in theory, be targeted to men involved in high-risk sexual behavior. Prophylactic vaccination against HPV infection10 is now being evaluated in clinical trials and could substantially reduce the rates of HPV infection and associated cervical cancers. Whether interventions intended to increase the rates of circumcision are a realistic and quantitatively important [and in the case of infant circumcision, ethical] addition to other strategies to combat cancer of the cervix remains to be documented. [But that didn't stop the circumcisors. Within days of the publication of this article, news items claiming not just a correlation but a causal relationship between intactness and cancer, and promoting (infant) circumcision, appeared in newspapers and magazines around the world.] Hans-Olov Adami, M.D., Ph.D. Dimitrios Trichopoulos, M.D., Ph.D. |
Back to the Intactivism index page.
{kind=link}
{kind=link}
{kind=link}
{kind=link}